Evidence with impact
Clinical studies show GammaTile consistently delivers outcomes that matter for patients with operable brain tumors.
A growing body of
peer-reviewed studies shows
consistent results:
Strong local tumor control and low rates of radiation necrosis for patients with operable brain tumors. Explore the evidence that’s shaping the future of brain tumor radiation therapy.1-8
GammaTile® clinical evidence:
Proven local control (LC) and
low rates of radiation necrosis (RN)
Safety and efficacy data review:
| Recurrent Meningioma | ||
| Study | Brachman 2018 PMID: 30,579,269 | |
| Study Design | Prospective | |
| # Patients | 19 | |
| # Treated Tumors | 20 | |
| Tumor Type | Meningioma (Recurrent) | |
| Efficacy Outcome | Median OS: 26 mos. 89% PFS at 18 mos. | |
| Safety | 10% RN 10% Pts with Surgical Complications | |
| Study | Study Design | # Patients | # Treated Tumors | Tumor Type | Efficacy Outcome | Safety |
|---|---|---|---|---|---|---|
| Newly Dx & Recurrent Brain Mets (BM) | ||||||
| Beckham 2025 | Retrospective | 31 | 38 | BM (Recurrent) | 87% LC at 12 mos. 94% LC at 12 mos. with GTR | 8% Symptomatic RN 2.6% Infection 12.9% LMD |
| Zeller 2024 PMID: 39429969 | Prospective (Registry) | 28 | 30 | Brain Mets (Newly Dx) | NR (Perioperative safety analysis) | Serious AE: 3.6% Total AE: 21.4% No AE was definitively related to GammaTile |
| Dharnipragada 2023 PMID: 37,324,216 | Retrospective | 10 | 10 | Rapidly Growing Brain Mets (Newly Dx & Recurrent) | 100% LC at median follow up of 6.2 mos. | No RN No Surgical Complications |
| Kutuk 2023 PMID: 37,722,990 | Retrospective | 10 | 12 | Brain Mets (Recurrent) | 100% LC at 6, 12, and 18 mos. | 8% Symptomatic RN |
| Imber 2022 PMID: 35,896,906 | Prospective | 20 | 25 | Brain Mets (Recurrent) | 92% LC at 12 months | 16% Symptomatic RN |
| Nakaji 2020 PMID: 33,224,684 | Prospective | 11 | 16 | Brain Mets (Newly Dx & Recurrent) | 83% LC at 12 mos. Newly Dx (n=4): 100% LC at 12 mos. Recurrent (n=12): 80% LC at 12 mos. | 12.5% Radiation Brain Changes Newly Dx (n=4) = 0% Recurrent (n=12) = 12.5% |
| Newly Dx & Recurrent Glioblastoma | ||||||
| Yekula 2024 PMID: 38281303 | Prospective | 7 | 7 | Rapidly Growing GBM (Newly Dx & Recurrent) | Median OS Newly Dx (n=3): 11.5 mos. Recurrent (n=4): 10 mos. Median PFS (All): 10.6 mos. | No RN No Surgical Complications |
| Smith 2022 PMID: 36,322,102 | Prospective | 28 | 28 | Glioblastoma (Recurrent) | Median time to LF: 12.1 mos. Median OS: 25.0 mos. Median PFS: 11.7 mos. | 7% Symptomatic RN |
| Gessler 2022 PMID: 35,088,050 | Prospective | 22 | 22 | IDH Wild-type Glioblastoma (Recurrent) | 86% LC at 6 mos. 81% LC at 12 mos. Median OS: 24.4 mos. Median PFS: 8.2 mos. | No RN 9% Pts with Surgical Complications |
| Recurrent Meningioma | ||||||
| Brachman 2018 PMID: 30,579,269 | Prospective | 19 | 20 | Meningioma (Recurrent) | Median OS: 26 mos. 89% PFS at 18 mos. | 10% RN 10% Pts with Surgical Complications |
LC = Local Control, LF = Local Failure, LMD = Leptomeningial Disease, NR = Not Reported, PFS = Progression-Free Survival, RN = Radiation Necrosis
Adapted from Garcia MA, et al. J Neurooncol. 166:203-212 (2024).
Proven local control:Proven
local control:
100% LC with 12 previously irradiated
brain mets | clinical and dosimetric evidence
Clinical evidence: 100% LC at 6, 12 and 18 months |
n = 12 tumors1
Kutuk T, et al. Brachytherapy 2023.
Dosimetric evidence: retrospective dosimetric
review of radiation treatment options:
recurrent brain mets | n = 12 tumors9
Kutuk T, et al. Brachytherapy 2024.
Axial illustration demonstrating the differences in biologically effective dose (BED) distribution amongst the radiation modalities
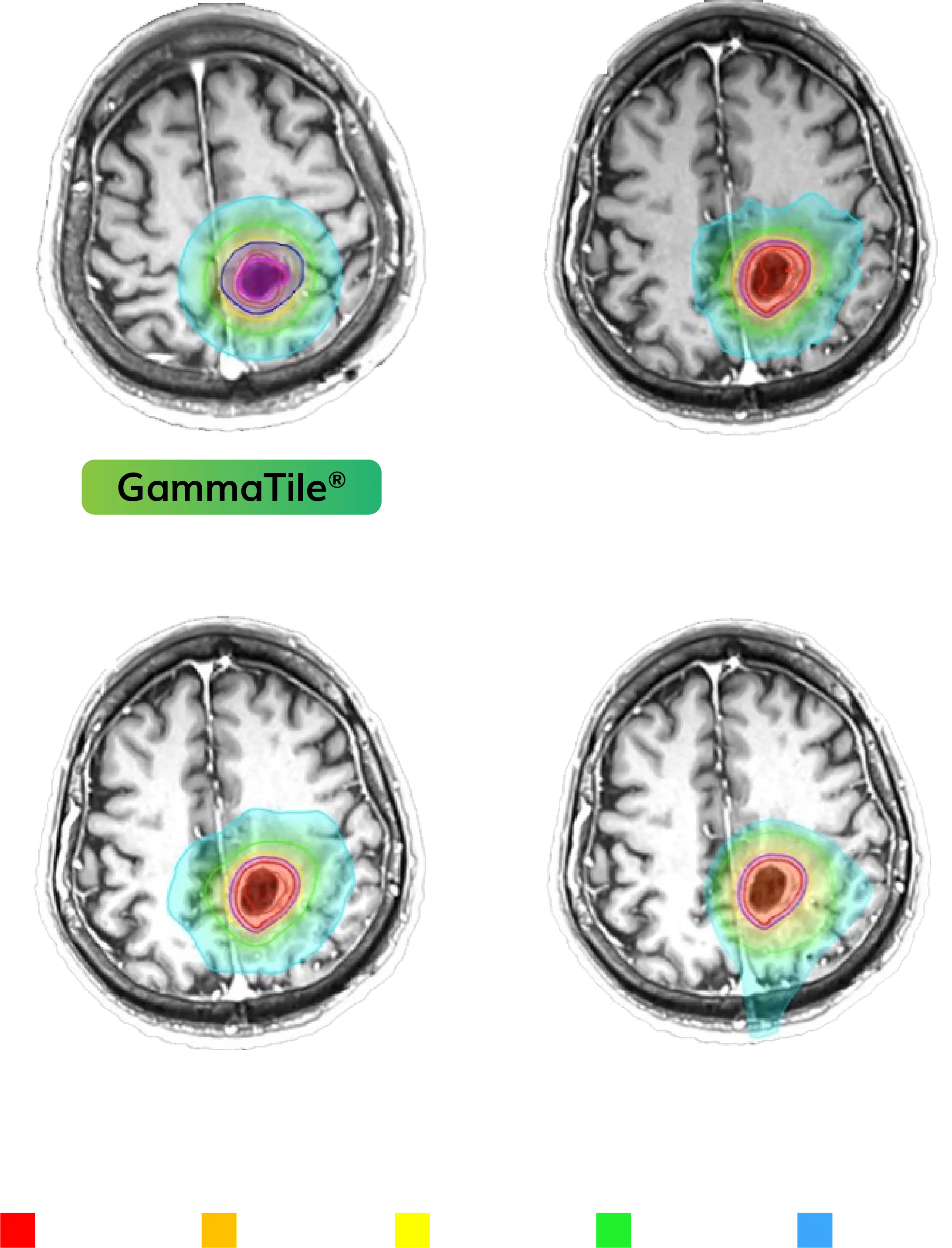
Images courtesy of Miami Cancer Institute.
BED10Gy90% Median
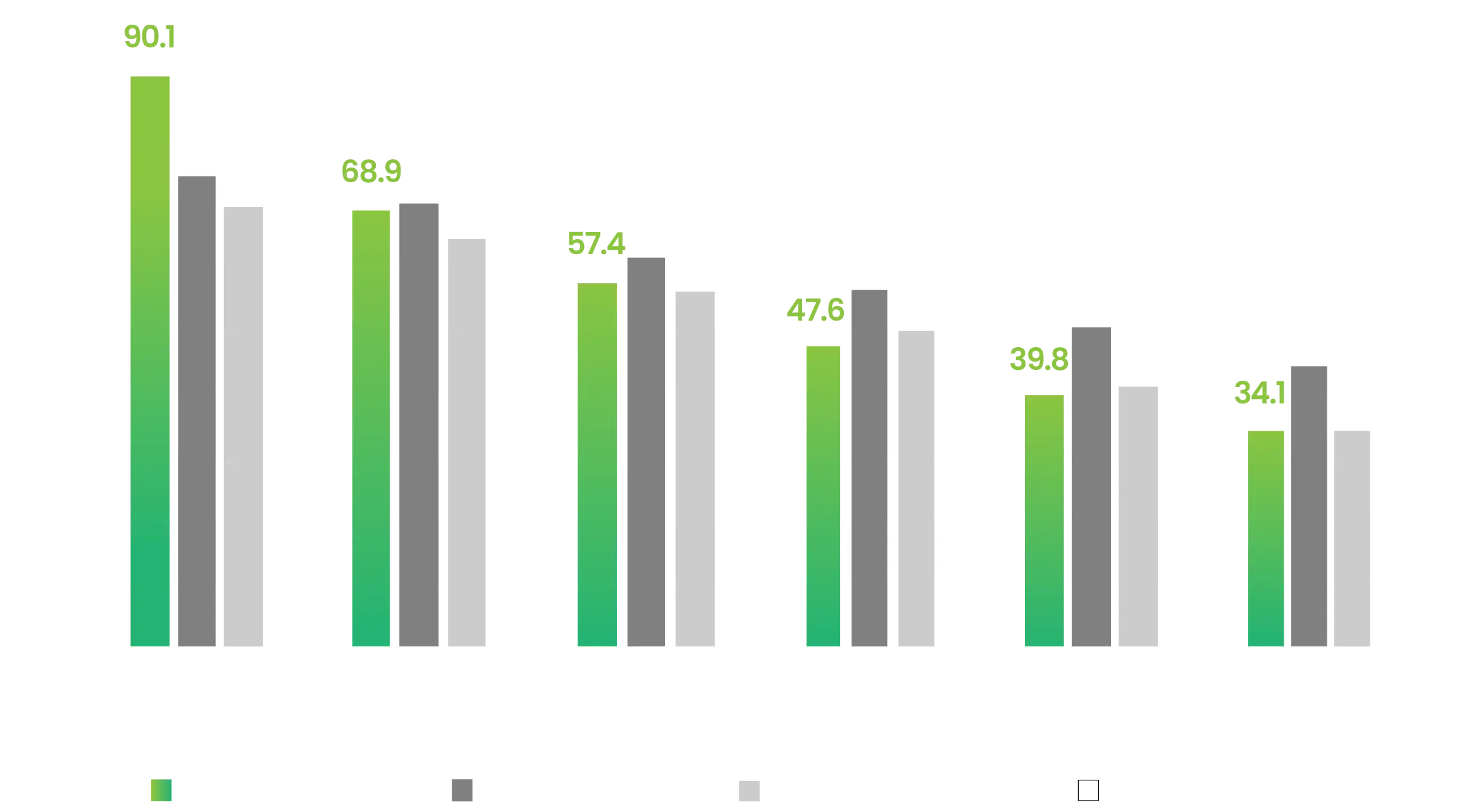
Key Insights
- GammaTile delivers statistically significant higher biologically effective dose (BED) at the resection cavity (RC) than other modalities (CyberKnife®, p = 0.04, Gamma Knife®, p = 0.005, Proton Therapy, p = 0.003).
- GammaTile’s BED was significantly lower 5mm away from the RC as compared to CyberKnife® (p = 0.045) and proton therapy (p = 0.03).
- Dose metrics associated with RN are significantly lower for GammaTile on pairwise comparisons (all p <0.05).
The GammaTile Commitment Pledge
for recurrent brain tumors
If a GammaTile treatment of a recurrent brain tumor is canceled because intraoperative pathology reveals only necrotic tissue, we will update the invoice to reflect a $0 charge.**