Brachytherapy
reimagined
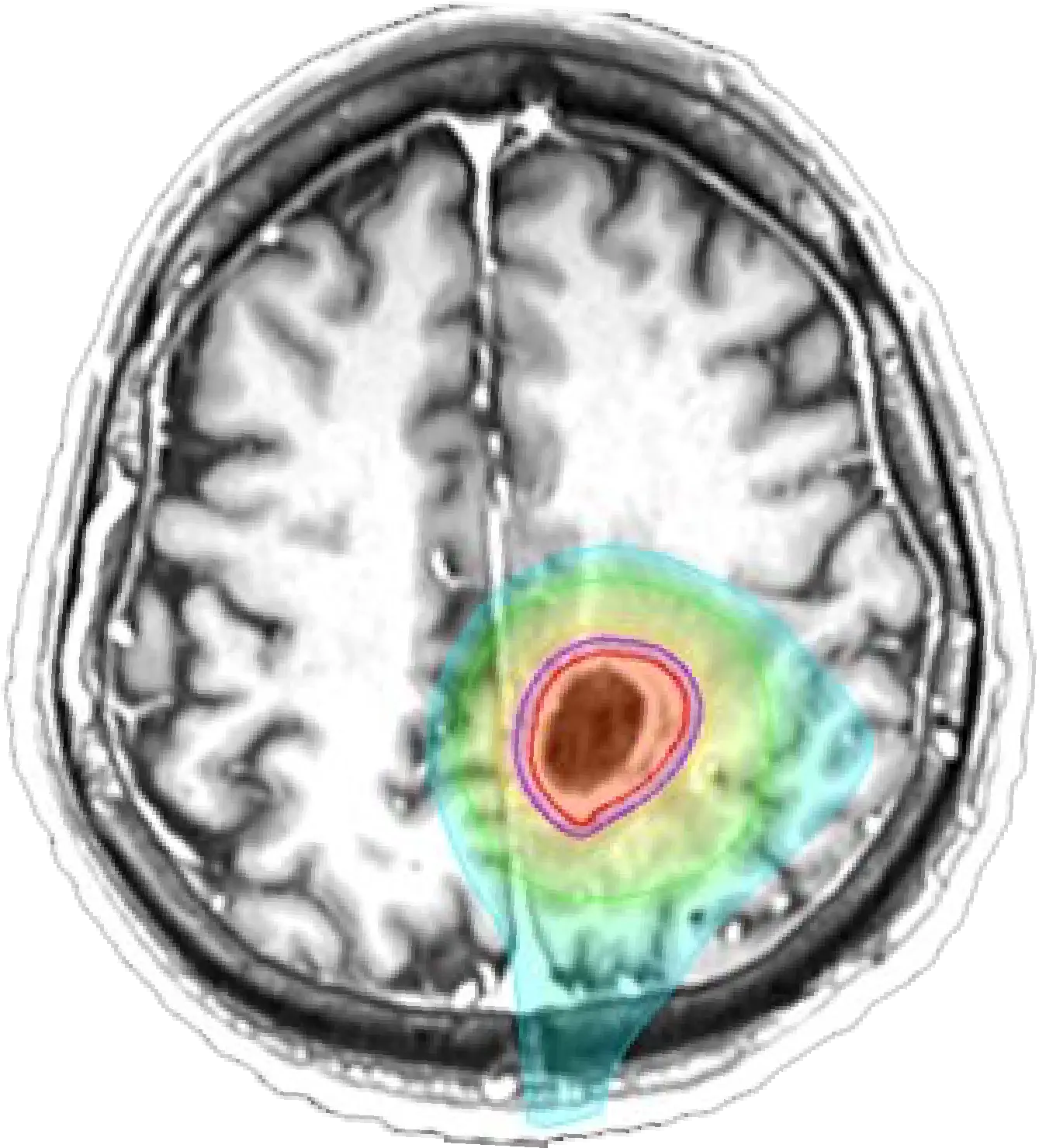
GammaTile® is a bioresorbable collagen implant embedded with four cesium-131 (Cs-131) seeds that delivers therapeutic radiation dose to the tumor cavity, while limiting the dose to healthy brain tissue.1
| Feature | GammaTile (with Cs-131)2 | Traditional Brachytherapy (with Iodine-125)2 | Benefit of GammaTile2 |
|---|---|---|---|
| Half-life | 9.7 days | 59.4 days | Shorter treatment duration, faster radiation delivery |
| Radiation Dose Delivery | Completes 88% in 30 days3 | Completes 88% in 184 days3 | Faster therapeutic effect |
| Reoperation Related to Radiation Necrosis (RN) | 0% reported in peer-reviewed publications3-10 Of the published RN, all have been medically managed3-10 | Up to 50% | Of the published GammaTile-related RN, all have been medically managed2-9 |
| Maximum dose of radiation (Dmax) to brain tissue | Minimal due to eliminating direct contact of the seeds with the adjacent brain tissue and uniform source spacing due to the structural collagen matrix | High risk due to direct contact of seeds with adjacent brain tissue and uneven seed distribution | Reduces Dmax to brain tissue with structural offset and uniform seed spacing |
| Long-term Radiation Exposure | Reduced due to rapid decay of Cs-131 | Significant due to prolonged exposure from ~60-day half-life | Eliminates extended exposure with rapid dose delivery |
| Dosimetry Predictability | Uniform radiation-source spacing helps give predictable, therapeutic radiation dose | Moderate precision, requires more planning | Reliable, efficient planning and outcomes with the collagen matrix, and marked reproducibility from patient to patient |
| Seed Migration | Fixed within a bioresorbable collagen matrix | Higher risk of migration reported in studies | Significantly reduces risk of migration with secure tile design |
| Staff Radiation Exposure | Minimal: preloaded tiles minimize handling time | Prolonged due to longer implantation times and potentially longer hospital stays | Tile design limits staff radiation exposure |
| Applications | Ideal for localized CNS tumors | Broader tumor beds, but with more potential side effects | More precise for localized tumor control |
| Feature | GammaTile (with Cs-131)2 | Traditional Brachytherapy (with Iodine-125)2 |
|---|---|---|
| Half-life | 9.7 days | 59.4 days |
| Radiation Dose Delivery | Completes 88% in 30 days3 | Completes 88% in 184 days3 |
| Reoperation Related to Radiation Necrosis (RN) | 0% reported in peer-reviewed publications3-10 Of the published RN, all have been medically managed3-10 | Up to 50% |
| Maximum dose of radiation (Dmax) to brain tissue | Minimal due to eliminating direct contact of the seeds with the adjacent brain tissue and uniform source spacing due to the structural collagen matrix | High risk due to direct contact of seeds with adjacent brain tissue and uneven seed distribution |
| Long-term Radiation Exposure | Reduced due to rapid decay of Cs-131 | Significant due to prolonged exposure from ~60-day half-life |
| Dosimetry Predictability | Uniform radiation-source spacing helps give predictable, therapeutic radiation dose | Moderate precision, requires more planning |
| Seed Migration | Fixed within a bioresorbable collagen matrix | Higher risk of migration reported in studies |
| Staff Radiation Exposure | Minimal: preloaded tiles minimize handling time | Prolonged due to longer implantation times and potentially longer hospital stays |
| Applications | Ideal for localized CNS tumors | Broader tumor beds, but with more potential side effects |
| Feature | GammaTile (with Cs-131)2 | Benefit of GammaTile2 |
|---|---|---|
| Half-life | 9.7 days | Shorter treatment duration, faster radiation delivery |
| Radiation Dose Delivery | Completes 88% in 30 days3 | Faster therapeutic effect |
| Reoperation Related to Radiation Necrosis (RN) | 0% reported in peer-reviewed publications3-10 Of the published RN, all have been medically managed3-10 | Of the published GammaTile-related RN, all have been medically managed2-9 |
| Maximum dose of radiation (Dmax) to brain tissue | Minimal due to eliminating direct contact of the seeds with the adjacent brain tissue and uniform source spacing due to the structural collagen matrix | Reduces Dmax to brain tissue with structural offset and uniform seed spacing |
| Long-term Radiation Exposure | Reduced due to rapid decay of Cs-131 | Eliminates extended exposure with rapid dose delivery |
| Dosimetry Predictability | Uniform radiation-source spacing helps give predictable, therapeutic radiation dose | Reliable, efficient planning and outcomes with the collagen matrix, and marked reproducibility from patient to patient |
| Seed Migration | Fixed within a bioresorbable collagen matrix | Significantly reduces risk of migration with secure tile design |
| Staff Radiation Exposure | Minimal: preloaded tiles minimize handling time | Tile design limits staff radiation exposure |
| Applications | Ideal for localized CNS tumors | More precise for localized tumor control |
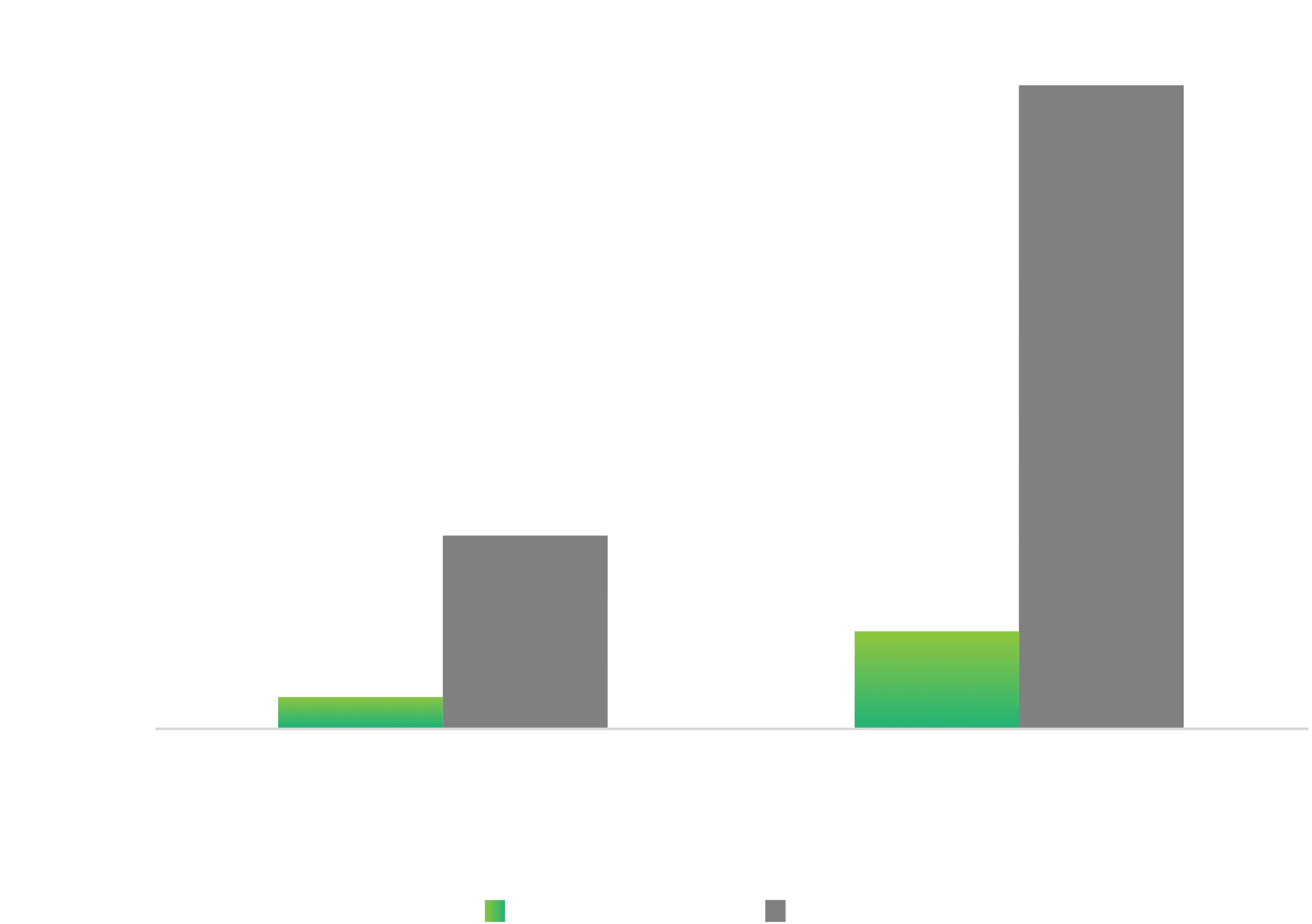
GammaTile vs. traditional brachytherapy:
the difference is the source: Cs-1312,3
GammaTile doesn’t just treat brain tumors —
it transforms how they are treated.
By combining cutting-edge radiation technology with surgical precision and a patient-focused approach, GammaTile sets a new brachytherapy standard for effectiveness, safety, and efficiency in brain tumor care.2,11